1918 Today
Preparing for the Next Pandemic
Preparing for the Next Pandemic
Introduction
This year marks the 100th anniversary of the 1918 influenza pandemic, also known as the “Spanish Flu”, which killed approximately 50 million people worldwide. This is the fourth and final installment of 1918 Today, Metabiota’s analysis of the most significant pandemic in modern history and what it can teach the world about how to prepare for devastating pandemics in the future. In our concluding installment, we will explore how influenza pandemic preparedness has evolved and discuss the many ways researchers and public health officials are striving to mitigate the impact of the next "Big One".
The Past
In 1918, the public health community and authorities had few tools to reduce the spread of the pandemic or lessen its impact. Surveillance, which we discussed in a previous 1918 Today installment, was practically non-existent and hindered by WWI. Attempts to reduce pandemic spread were sporadic at best and done through school closures, cancellation of public gatherings, isolation and quarantine. The lack of scientific knowledge also hindered the ability to reduce the impact and spread of the pandemic (the influenza virus was not discovered until the 1930s) on top of a healthcare system that was still in its infancy.
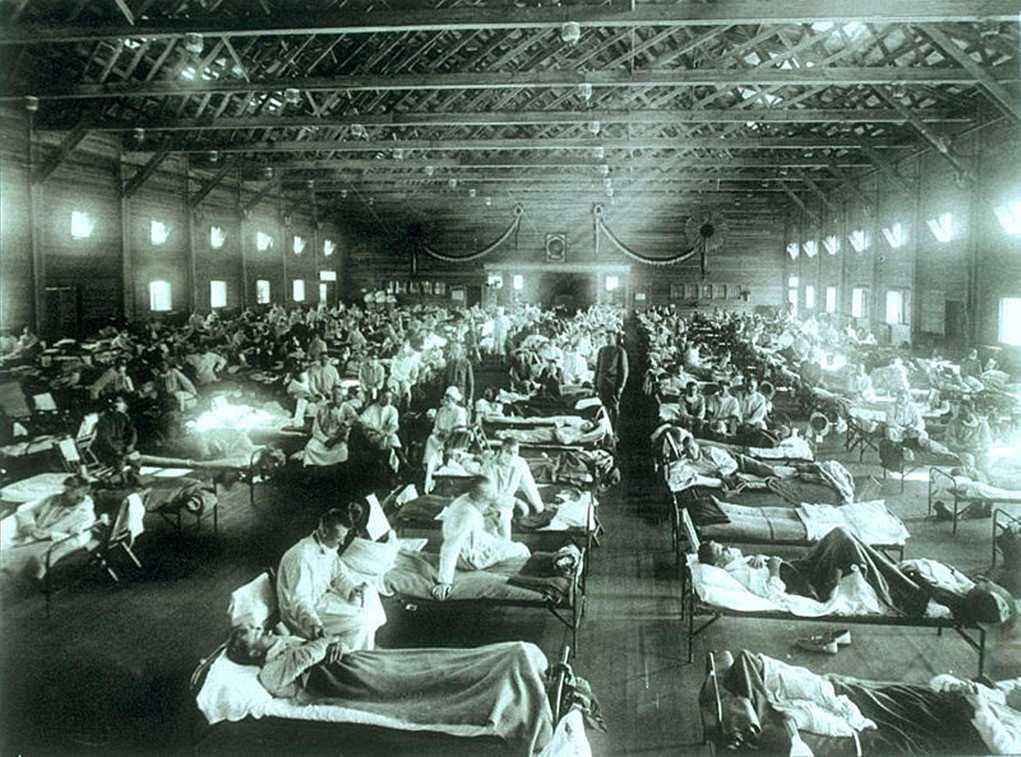
One hundred years ago, the majority of pandemic-related deaths were due to bacterial pneumonia, which can develop after the initial influenza virus infection. Without drugs to target either the influenza virus or secondary bacterial infections, clinicians relied upon supportive care and post-hoc response plans for surge capacity (Figure 1).

{kind=link}
The Present
Pandemic preparedness has come a long way since the "Spanish Flu". Key advancements (while not exhaustive) are summarized in the box below:
Advancements in influenza preparedness:
- Detection. Improved discovery of the influenza virus in humans and animals (1933 and 1930 respectively), and the ability to rapidly differentiate between viral strains.
- Prevention. Development of an influenza vaccine in the 1940s.
- Treatment. Introduction of several antiviral drugs, including neuraminidase inhibitors and a new class of drugs that can stop the influenza virus from replicating. Additionally, bacterial pneumonia now is largely treatable through antibiotics.
- Surveillance and Global Cooperation. With the Development of International Health Regulations (IHR), Global Health Security Agenda (GHSA), and national influenza pandemic preparedness plans, efforts to uncover viruses and mitigate their spread has improved greatly.
To respond to the next pandemic, it needs to first be detected. The World Health Organization's (WHO) Global Influenza Programme provides global standards for influenza surveillance. Regular sharing of influenza data (e.g., what strains are circulating) between countries allows scientists to detect the emergence of a novel virus.
The IHR outlines the role of the WHO and each Member State during an international influenza pandemic. The Pandemic Influenza Preparedness framework was revised in 2017 and provides guidance on communication between the Member States, the WHO, the healthcare sector, and the public, which has been of immense importance in previous pandemics including the 2009 influenza pandemic. It also tries to ensure predictable, efficient and equitable access to vaccines and medicines for countries in need.
Metabiota has developed an Epidemic Preparedness Index that measures and assesses the preparedness of 188 countries to detect, communicate about, and respond to epidemic or pandemic events (Figure 2). Some specific measures include public health communications, health and economic resources, bureaucratic and public management capacities, and infrastructure. This tool helps to identify the geospatial gaps for pandemic preparedness, monitor changes in preparedness, and to understand which countries would benefit from increased resource allocation or capacity-building activities.

The Future
Seasonal influenza occurs every year and influenza pandemics have occurred about every 33 years on average. With that in mind, researchers have put considerable effort towards developing an influenza vaccine that would protect against a broad array of influenza strains. This vaccine would ideally confer long-term immunity to all influenza A virus subtypes and could be produced all year long, thus increasing pandemic stockpiles and the global vaccine supply. Universal influenza vaccine development efforts are expected to increase in the future; the March 2018 US federal spending bill included $100 million for the development of a universal influenza vaccine.
The continued refinement of infectious disease modeling and forecasting capabilities will also support pandemic response activities. Health care organizations and other businesses will be better able to plan and prepare for surges of influenza cases or increases in employee absenteeism. Additionally, the increased accessibility and democratization of tools like 3D printers provide novel opportunities for increasing preparedness by creating on-demand personal protective equipment.
While many trends are promising for greater preparedness, there are also several factors which could derail the response to the next pandemic. Political instability, armed conflict, and natural disasters can sabotage response activities and amplify pandemic impacts. Lack of effective and transparent population health messaging and risk communication during a pandemic can result in ineffective behavioral responses that are driven by fear and decreased trust.
Antivirals can effectively treat influenza infections, but over time, viruses may become resistant. Furthermore, while antibiotics are easily accessed in the present day, warning bells have been sounding for years about the rise of antibiotic-resistant bacterial infections. The limited research investment into new antibiotics and the continued overuse of these drugs pose a risk to the future treatment of secondary bacterial infections occurring during an influenza pandemic, as bacterial resistance can render antibiotics useless.
The future of effective global pandemic preparedness relies not only on the development and implementation of new technologies but also on continued investment in strengthening national public health capacity and infrastructure, data sharing and communication. Pandemic preparedness planning efforts also require constant review and evaluation, identification of potential risks and gaps, and continued application of lessons learned. Most of all, these efforts require strong cooperation across sectors and between local, national and global members.
Responsibility for preparing for the next “Big One” ultimately falls on all parties and organizational levels.
The Takeaways
- One hundred years ago, limitations in our scientific understanding of influenza hindered our capacity to reduce the spread and mitigate the impact of the 1918 pandemic.
- Over the last century, there have been great strides in pandemic preparedness through improved detection, prevention, treatment, and cooperation.
- Future preparedness depends on scientific and technological advancements in addition to expanding surveillance and planning activities.
- The next “Big One” can be exacerbated by drug resistance, political instability, armed conflict, and natural disasters.
Metabiota thanks all of you readers for your interest and engagement in this topic throughout 2018. We welcome your comments and feedback on new features and topics in 2019. Please visit this link to submit your ideas.
Previous Installments of 1918 Today
Contact Information

Find us here: Metabiota Health, 535 Mission St
14th Floor
San Francisco
CA
94105
USA
Email: [email protected]
Phone: (415) 398-4712